
หน้าหลัก | สุขภาพดี | สุภาพสตรี | การแปลผลเลือด | โรคต่างๆ | ยารักษาโรค |วัคซีน | อาหารเพื่อสุขภาพ

What is a macular hole?
The eye is often compared to a camera. The front of the eye contains a lens that focuses images on the inside of the back of the eye. This area, called the retina, is covered with special nerve cells that react to light, like film in a camera. These nerve cells are very close together in the middle of the retina where the eye focuses the images that we see. This small part of the retina is called the macula.
Sometimes the nerve cells of the macula become separated from each other and pull away from the back surface of the eye forming a hole. This is called a macular hole.
Why do people get macular holes?
Sometimes macular holes are the result of an injury or a medical condition that affects the eye, including being very near sighted. In most people, it is due to traction on the center of vision that is more likely to occur as we age.
How does a doctor know whether someone has a macular hole?
The symptoms of macular hole include:
When these symptoms are caused by a macular hole, they will occur in only the eye with the macular hole. It is very rare for someone to have macular holes in both eyes.
If any of these symptoms occur, it is important to schedule an appointment with your doctor as soon as possible. The doctor will use a special instrument to look inside the eye and see whether the macula has a hole in it.
To diagnose a macular hole, your doctor will perform special imaging tests calledoptical coherence tomography that gives them a cross sectional view of your retina. This tests helps diagnose a macular hole and can differentiate it from other diagnosis that may appear similar.
Is there any treatment for macular hole?
Rarely, your doctor might recommend not treating a macular hole if it is small, if it does not cause severe vision problems, and if the eye is otherwise healthy in all other ways. The doctor might just recommend that you have eye examinations more frequently to make sure that the macular hole does not get any larger or cause other problems. It is important to keep these appointments because although the macular hole might not get worse for a while, it will almost never go away by itself.
If your vision is decreased and the macular hole is small, your doctor may recommend the use of a drug that is injected into the eye. This drug helps dissolve the traction that caused the macular hole and allows the hole to close in about half of the cases. The injection is not painful as the eye is numbed before the injection is performed. Not everyone is a candidate for this injection so check with your doctor.
If your vision is decreased and the macular hole is large then your doctor will often recommend that the macular hole be treated with surgery.
What happens in the operation to treat a macular hole?
The surgical procedure for macular holes is performed under local anesthetic so the patient is awake but does not feel the procedure.
The first part of the operation for macular hole treatment is to remove this gel-like material, which is called the vitreous. The procedure to remove it is called a vitrectomy.
The surgeon will make small openings in the eye to insert special instruments that are used to remove the vitreous. The surgeon may also remove any small pieces of tissue ("membranes") or traction near the macular hole using fine forceps. This is done to prevent anything from pulling on the macula preventing the hole from closing.
Finally, the fluid in the eye is exchanged with a sterile gas, which keeps pressure on the macular hole until it heals. Patients will need to maintain a face-down position for 1 to 7 days to keep the gas bubble in place and help close the hole.
How successful is surgery to repair macular holes?
Surgery is successful in closing the hole in more than 90 percent of patients. However, the success rate is closer to 60 percent if face-down position is not maintained. The amount of vision that typically is regained varies. Ask your doctor about the amount of visual improvement you might expect.
References:
What Is a Macular Hole?
A macular hole is a small break in the macula, the part of your eye responsible for detailed, central vision.
The macula is a very small area at the center of the retina — a thin layer of light-sensitive tissue that lines the back of the eye. Light rays are focused onto the retina, where they are transmitted to the brain and interpreted as the images you see. It is the macula that is responsible for your pinpoint vision, allowing you to read, sew or recognize a face.
As we grow older, the thick vitreous gel in the middle of our eyes shrinks and pulls away from the macula. If the gel sticks to the macula and doesn't pull away, the macular tissue stretches and eventually tears, forming a hole.
If you have macular hole symptoms, you will have blurred and distorted central vision.
What Causes a Macular Hole?
Your eye is filled with a gel-like substance called vitreous, which lies in front of the macula. As you age, the vitreous gel shrinks and pulls away from the macula, usually with no negative effect on your sight. In some cases, however, the vitreous gel sticks to the macula and is unable to pull away. As a result, the macular tissue stretches. After several weeks or months the macula tears, forming a hole.
Macular holes are associated with aging and usually occur in people over the age of 60. Less common causes of macular holes include injury to the eye and long-term swelling of the macula.
Macular Hole Symptoms
In the early stages of macular hole formation, symptoms may not be completely obvious. Your central vision becomes blurred and distorted. If the hole progresses, a blind spot develops in your central vision and impairs the ability to see at both distant and close range. Symptoms of macular hole usually occur in one eye only, as it is uncommon to have a macular hole in both eyes.
Macular hole symptoms include:
If any of these symptoms occur, it is important to schedule an appointment with your eye doctor as soon as possible. Your ophthalmologist will use a special instrument to look inside the eye and see whether the macula has a hole in it.
It is important to note that if the macula is damaged, you will not lose your vision entirely. You will still have peripheral, or side, vision.
Macular Hole Diagnosis
During an eye exam, your ophthalmologist will dilate your pupils and examine your retina. You may have a test called fluorescein angiography that uses dye to illuminate areas of the retina.
Another test called optical coherence tomography (OCT) is most helpful in making an accurate macular hole diagnosis. With OCT, a special diagnostic laser camera is used to photograph your retina. It measures the thickness of the retina and is also very sensitive at detecting swelling and fluid. OCT can also diagnose small macular holes that are too small to be seen in an examination or with angiography.
Macular Hole Treatment
Vitrectomy surgery is the most effective treatment to repair a macular hole and possibly improve vision.
Macular hole surgery involves using tiny instruments to remove the vitreous gel that is pulling on the macula. The eye is then filled with a special gas or oil bubble to help flatten the macular hole and hold the retinal tissue in place while it heals.
If you have vitrectomy surgery, you must maintain a constant face-down position after surgery to keep the bubble in contact with the macula to allow effective healing. This can range from a few days to a few weeks, depending on your surgeon’s recommendation and the size of your hole. A successful result often depends on how well this position is maintained. The bubble will then slowly dissolve on its own, or, in some cases, be removed by your ophthalmologist.
If you have a gas bubble, you cannot fly in an airplane until the gas bubble has dissolved, as a rapid increase in altitude can cause a dangerous rise in eye pressure. You must also not undergo general anesthesia using nitrous gas, though it is generally safe to have general anesthesia without using nitrous gas.
As the macular hole closes, the eye usually regains some of the lost sight. How much vision is restored generally depends on the size of the hole and how long it was present before surgery.
การทำงานของตา
Background
A macular hole is a defect of the foveal retina involving its full thickness from the internal limiting membrane (ILM) to the outer segment of the photoreceptor layer.
See the image below.
 Full-thickness macular hole showing a surrounding cuff of subretinal fluid.
Full-thickness macular hole showing a surrounding cuff of subretinal fluid.A macular hole was first described by Knapp in 1869 in a patient who sustained blunt trauma to the eye. Subsequent case reports and series pointed to antecedent episodes of ocular trauma such that the two were customarily linked to each other. However, throughout this century, ophthalmologists increasingly have recognized that this condition more commonly occurs in atraumatic settings and have differentiated these macular holes from trauma-induced holes by describing them as idiopathic full-thickness macular holes. In fact, case series as far back as the 1970s reported that more than 80% of macular holes are idiopathic and that only less than 10% have associated history of trauma to the eye.
Pathophysiology
The causes underlying trauma-related macular holes and idiopathic macular holes are understandably divergent.
Trauma-related macular holes are suspected to be related to the transmission of concussive force in a contrecoup manner, which results in the immediate rupture of the macula at its thinnest point. Patients who underwent successful repair of arhegmatogenous retinal detachment were also found to infrequently develop macular holes (< 1% incidence). The underlying pathophysiology for formation of these holes is not well understood, though epiretinal membrane formation, foveal photoreceptor atrophy, and hydraulic forces may play a role.
While the vitreous was suspected to be involved in the causation of idiopathic macular holes by Lister in 1924, Johnson and Gass, in 1988, first described a classification system that focused on anteroposterior and tangential vitreous traction on the fovea as a primary underlying cause for idiopathic macular holes.[1, 2] Shrinkage of prefoveal cortical vitreous with persistent adherence of vitreous to the foveal region results in the causative traction.
Gass macular hole stages are described below.
Stage 1a (foveal detachment; macular cyst): Tangential vitreous traction results in the elevation of the fovea marked by increased clinical prominence of xanthophyll pigment. This stage is occasionally referred to as the yellow dot stage and can also be seen in cases of central serous chorioretinopathy, cystoid macular edema, and solar retinopathy as depicted below.
 Fundus photograph of a stage 1a macular hole with characteristic yellow spot at the center of the fovea.
Fundus photograph of a stage 1a macular hole with characteristic yellow spot at the center of the fovea.Stage 1b: As the foveal retina elevates to the level of the perifoveal, the yellow dot of xanthophyll pigment changes to a donut shaped yellow ring. Persistent traction on the fovea leads to dehiscence of deeper retinal layers at the umbo.
Stage 2: This is the first stage when a full-thickness break in the retina exists. It is defined as a full-thickness macular hole less than 400 µm in size. The full-thickness defect may appear eccentric, and there may be a pseudo-operculum at this stage if there has been spontaneous vitreofoveolar separation. These opercula have been examined and found to be vitreous condensation and glial proliferation without harboring any retinal tissue.
Stage 3: A full-thickness macular hole in the retina exists. It is greater than 400 µm in size and is still with partial vitreomacular adhesion/traction.
Stage 4: A full-thickness macular hole exists in the presence of a complete separation of the vitreous from the macula and the optic disc. There is evidence, however, that, even in the presence of an apparent posterior vitreous detachment, a thin shell of residual cortical vitreous may still remain and contribute to the macular hole.
The advent of ocular coherence tomography (OCT) has provided in vivo structural support to hypotheses focused on vitreous traction underlying idiopathic macular holes. The OCT has allowed careful evaluation of the vitreoretinal interface demonstrating persistent adhesion on the fovea resulting in oblique traction on the fovea even with a partial posterior vitreous detachment. The persistent traction on the fovea prior to anatomic changes to the fovea has been referred to as Stage 0. This clinical appearance may resolve without progression in 40-50% of patients.[3]
Visual dysfunction in patients with macular hole is directly related to the absence of retinal tissue in the fovea. However, visual dysfunction may seem out of proportion to the size of the macular hole and potentially may also be related to the presence of a cuff of subretinal fluid with associated photoreceptor atrophy.
See Causes.
Frequency
United States
The overall prevalence is approximately 3.3 cases in 1000 in those persons older than 55 years. Peak incidence of idiopathic macular hole development is in the seventh decade of life, and women typically are affected more than men. Reasons for this, at best, are speculative at this point. Some epidemiologic risk factors, such as cardiovascular disease, hypertension, and a history of hysterectomy, have been reported by other studies. However, none of these have been proven to have any significant association with macular hole formation.
International
The prevalence rate of macular hole in India is a reported 0.17%, with a mean age of 67 years.
The Beijing Eye Study found the rate of macular holes to be 1.6 out of 1000 elderly Chinese, with a strong female predilection.
Mortality/Morbidity
The natural history of a macular hole varies based on its current clinical stage. It has been reported that around 50% of stage 0 and stage 1 macular holes may resolve both in the anatomic changes and the symptoms produced. Stage 2 holes progress and worsen in most cases to stage 3 or stage 4, resulting in worsening vision. Best estimates for the incidence of development of an idiopathic full-thickness macular hole in the fellow eye are approximately 12%. In rare instances (0-10%), a full-thickness macular hole may spontaneously close with resultant good vision.
Race
There is no racial predilection reported, though prevalence rates for the epidemiologic studies in India and China are consistent with reported data.
Sex
Women typically are affected more than men.
Age
Peak incidence is in the seventh decade of life.
History
Patients with idiopathic macular holes present with a variety of symptoms.
Initial symptoms include blurred central vision or metamorphopsia. Patients may characterize these symptoms as being mild and only apparent when reading or driving. Because the initial changes may be mild and gradual, it may be some time before the patient discovers that something is wrong with their vision. Macular holes may only be discovered when patients cover one eye and notice blurred vision and metamorphopsia in the opposite eye.
Rarely, some patients may describe the exact moment at which the hole developed, but more commonly, they describe the onset as slow and gradual if at all noticeable.
Later, a larger macular hole may produce a central defect, or scotoma, in the central vision of the patient.
Some patients may be asymptomatic, and the hole is diagnosed only on routine ophthalmologic examination.
Physical
The visual acuity of the patient varies according to the size, location, and the stage of the macular hole. Patients with small, eccentric holes may retain excellent visual acuity in the range of 20/25 to 20/40. In addition, a macular hole that is not full thickness can have very good visual acuity in the range of 20/30 to 20/50. However, once a macular hole is well developed or full thickness, the usual range of visual acuity is from 20/80 to 20/400, averaging at 20/200.
Direct ophthalmoscopy
A full-thickness macular hole visualized with direct ophthalmoscopy is characterized by a well-defined round or oval lesion in the macula with yellow-white deposits at the base. These yellow dots probably represent lipofuscin-laden macrophages or nodular proliferations of the underlying pigment epithelium with associated eosinophilic material as shown below.
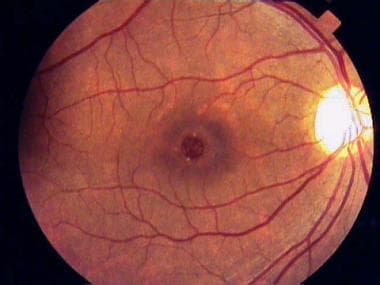 Full-thickness macular hole with typical yellowish granular deposits on the retinal pigment epithelium.
Full-thickness macular hole with typical yellowish granular deposits on the retinal pigment epithelium.Biomicroscopic (slit lamp) examination
With biomicroscopic (slit lamp) examination, a round excavation with well-defined borders interrupting the beam of the slit lamp can be observed.
In most patients, an overlying semitranslucent tissue, representing the pseudo-operculum, can be seen suspended over the hole. There is often a surrounding cuff of subretinal fluid as depicted below.
Full-thickness macular hole showing a surrounding cuff of subretinal fluid.Cystic changes of the retina also may be evident at the margins of the hole. The retinal pigment epithelium is usually intact and normal in acute stages but may undergo chronic changes, such as atrophy and hyperplasia, with time.
Fine crinkling of the inner retinal surface caused by an epiretinal membrane may be present and sometimes may even distort the appearance of the hole.
Watzke-Allen and the laser aiming beam tests
The most useful diagnostic tests for ophthalmologists to distinguish full-thickness macular holes from other lesions are the Watzke-Allen and the laser aiming beam tests.
The Watzke-Allen test is performed at the slit lamp using a macular lens and placing a narrow vertical slit beam through the fovea. A positive test is elicited when patients detect a break in the bar of light that they perceive. This reaction is due to the fact that there is a lack of retinal material in the area of the hole, thus producing a central defect or scotoma. Narrowing or distortion of the bar of light is not diagnostic of full-thickness macular holes and should be interpreted with caution.
The laser aiming beam test also is performed similarly, but this time a small 50-µm spot size laser aiming beam is placed within the lesion. A positive test is obtained when the patient fails to detect the aiming beam when it is placed within the lesion but is able to detect it once it is placed onto normal retina.
In addition, some slit lamps are equipped with a setting to project a small test object, often a star, onto the fovea. Again, the patient is asked whether they perceive the test object.
Trauma
Of patients experiencing a contusion injury of the eye, 6% develop a macular hole following the trauma.
Trauma is also commonly associated with commotio retinae involving the macula, subretinal hemorrhage, and intraretinal hemorrhage.
Progressive high myopia (foveal schisis)
Patients with high myopia may develop foveal schisis and/or lamellar holes, which can progress to a full-thickness macular hole.
Of those patients in whom foveal schisis identified, 31% developed macular holes.
Tanaka et al reviewed 24 eyes of 21 consecutive patients with lamellar holes and high myopia. Over a mean follow-up of 19.2 months, these lamellar macular holes remained very stable; only one eye progressed to a full-thickness macular hole.[4]
Risk factors include axial eye length, macular chorioretinal atrophy, and vitreoretinal interface factors.
Preceding rhegmatogenous retinal detachmen
Less than 1% of patients with a successfully repaired rhegmatogenous retinal detachment will present with a subsequent macular hole.
Vitreoretinal traction theory (idiopathic macular holes)
See Pathophysiology.
Vitreous syneresis results in shrinkage of cortical vitreous and traction on the fovea.
Diagnostic Considerations
Pseudohole due to epimacular membrane
Cystoid macular edema
Lamellar macular hole
Vitreomacular traction syndrome
Primary consideration should be given to conditions that may mimic the appearance of a macular hole. While most of these conditions are readily apparent clinically, subtle presentations may present as a macular hole. These conditions include any disease that can cause the development of cystoid macular edema (eg, choroidal neovascularization, retinal vein occlusions, retinitis pigmentosa). An appropriate work-up and examination should identify these conditions.
Differential Diagnoses
Ocular coherence tomography
Ocular coherence tomography (OCT) allows high-resolution cross-sectional imaging of the retina. OCT allows the physician to detect the presence of a macular hole as well as changes in the surrounding retina.
OCT can distinguish lamellar holes and cystic lesions of the macula from macular holes.
Also, the status of the vitreomacular interface can be evaluated. This allows the clinician to evaluate the earliest of the stages of a macular hole as well as evaluate for other vision-limiting conditions associated with macular holes, such as a surrounding cuff of subretinal fluid.
Fluorescein angiography
Fluorescein angiography (FA) may be a useful test in differentiating macular holes from masquerading lesions, such as CME and choroidal neovascularization (CNV).
Full-thickness stage 3 holes typically produce a window defect early in the angiogram and do not expand with time as depicted below. The arteriovenous phase of the angiogram best demonstrates a granular hyperfluorescent window associated with the overlying pigment layer changes.
 Fluorescein angiogram showing a central window defect.
Fluorescein angiogram showing a central window defect.No leakage or accumulation of dye is observed as opposed to other lesions.
In CME, a gradual accumulation of dye occurs in the cystoid spaces, eventually demonstrating a petaloid appearance late in the angiogram.
B-scan ultrasonography
B-scan ultrasonography may be helpful in elucidating the relationship of the macula to the vitreous; therefore, it may be helpful in staging the disease but is not sensitive to distinguish a true macular hole from masquerading lesions.
Amsler grid abnormalities, although sensitive for macular lesions, are not specific for macular holes. Plotting of small central scotomas caused by full-thickness macular holes using the Amsler grid is difficult because of the poor fixation in the affected eye. However, bowing of the lines and micropsia frequently are appreciated. This could be attributable to the surrounding area of retinal edema and intraretinal cysts, which could be seen in macular holes as well as other lesions like CNV.
Microperimetry and multifocal electroretinography have also been used to evaluate patients with idiopathic macular holes. These studies show loss of retinal function corresponding to the macular hole with subsequent recovery of function following surgical repair of the hole.
Medical Care
Case reports exist that describe the use of autologous plasmin for idiopathic and traumatic macular holes. Ongoing clinical trials are evaluating the role of plasmin as a means of “chemovitrectomy.” In these studies, case illustrations have demonstrated resolution of idiopathic macular holes following intravitreal injection of plasmin and no surgical intervention.
In October 2012, ocriplasmin (Jetrea) was approved by the US Food and Drug Administration (FDA) for the treatment of vitreomacular adhesion. Ocriplasmin is a recombinant proteolytic enzyme that underwent study by the MIVI-TRUST study group. This protease demonstrated activity against fibronectin and laminin. In a randomized, double-blind study, 652 eyes with vitreomacular adhesion were treated with an intravitreal injection of ocriplasmin. A secondary endpoint of the study was nonsurgical closure of a full-thickness macular hole, which can result from vitreomacular adhesion. In the study, 40.6% of treated eyes experienced nonsurgical closure of the macular hole compared to 10.6% in the placebo group (P< 0.001). FDA approval was based on this study. This injectable medication provides a nonsurgical means of treating macular holes.[5]
There are concerns with the potential for retinal toxicity from the use of ocriplasmin (See Medication below).
The potential for better vision, as well as the 12% chance that the fellow eye will develop another macular hole, has prompted ophthalmologists to seek for a viable treatment of this condition.
Indications for consideration of the surgical management of macular holes are based on the presence of a full-thickness defect. Once this defect has developed, the potential for spontaneous resolution is low. Thus, surgical management is recommended with documentation of a stage 2 or higher, full-thickness macular hole. Stage 1 holes and lamellar holes are managed conservatively with observation at this time. See Controversies surrounding the surgical repair of macular holes.
Historically, therapy for macular holes has evolved from pharmacologic interventions, such as anxiolytics and vasodilators, to an assortment of surgical techniques, such as cerclage, scleral buckles, direct photocoagulation of the hole edges, and intraocular gas tamponade without the aid of vitrectomy. In 1982, Gonvers and Machemer were the first to recommend vitrectomy, intravitreal gas, and prone positioning for retinal detachments secondary to macular holes.[6]
Kelly and Wendel reported that vision might be stabilized or even improved if it were possible to surgically relieve tangential traction on the macula, reduce the cystic changes, and reattach the cuff of detached retina surrounding the macular hole.[7] They proposed that by performing this surgery, they could flatten the retina and possibly reduce the adjacent cystic retinal changes and neurosensory macular detachment.[7]
In 1991, Kelly and Wendel demonstrated that vitrectomy, removal of cortical vitreous and epiretinal membranes, and strict face-down gas tamponade could successfully treat full-thickness macular holes.[7] The overall results of their initial report were a 58% anatomic success rate and visual improvement of 2 or more lines in 42% of eyes. A succeeding report showed a 73% anatomic success rate and 55% of patients improving 2 or more lines of visual acuity. Present anatomic success rates range from 82-100% depending on the series.
A prospective, randomized, and controlled series by the Vitrectomy for Treatment of Macular Hole Study Group for stage 2, 3, and 4 holes showed that vision was improved in surgically treated eyes compared with observed eyes. However, more frequent adverse effects were observed in the surgically treated eyes compared to the control eyes, with the most common adverse effects being macular retinal pigment epithelium changes and cataractogenesis.
Some aspects of the surgery may vary, but the basic technique is the same. The anterior and middle vitreous is removed via a standard 3-port pars plana vitrectomy. Patients with macular hole frequently undergo vitrectomy using smaller gauge vitrectomy systems (ie, 25 gauge, 23 gauge). Associated instruments have been developed for these smaller gauge, transconjunctival vitrectomy systems.
The critical step appears to be the removal of the perimacular traction. Factors contributing to this traction, such as the posterior hyaloid, the ILM, and coexisting epimacular membranes, need to be addressed. The traction exerted by the posterior hyaloid on the macula should be relieved by either removing just the perimacular vitreous or combining it with the induction of a complete posterior vitreous detachment. Various surgical techniques have been described to accomplish this task, including the use of a soft-tipped silicon cannula or the vitrectomy cutter with the cutter disengaged. A "fish-strike sign" or bending of the silicon cannula has been described as a sign that the posterior hyaloid has been engaged. Then, it may be released from the underlying retina and removed with the vitrectomy cutter.
The removal of ILM is considered to be a contributing factor in the success of macular hole surgeries. ILM peeling may be accomplished via a "rhexis" not unlike that of a capsulorrhexis in lens surgeries. Very fine forceps may be used to peel the ILM from the underlying retina. Care should be taken not to include the deeper layers in the forceps' grasp, which may further damage the surrounding retinal tissues. Currently, many surgeons use indocyanine green dye to stain the ILM making it easier to visualize and manipulate.
Epiretinal membranes, if present, also should be removed. Techniques in completing this procedure vary from surgeon to surgeon.
After careful indirect ophthalmoscopic examination of the peripheral retina for tears, a total air-fluid exchange is performed to desiccate the vitreous cavity. A nonexpansile concentration of a long-acting gas is exchanged for air. Studies have shown that a longer period of internal tamponade equated to a higher success rate.
Sterile air and varying concentrations of either perfluoropropane or sulfur hexafluoride have been used based on surgeon preference for internal tamponade. The primary difference achieved using different gases is the duration of the gas bubble and, consequently, the amount of internal tamponade achieved within the first several days after surgery. Silicone oil has also been used as an internal tamponade for patients with difficulty positioning or altitude restrictions. However, the use of silicone oil necessitates a second subsequent surgery to remove the oil. Furthermore, the visual results are not comparable to the use of gas tamponade, possibly as a result of silicone oil toxicity at the level of the photoreceptors and RPE.
Tafoya et al showed, at 1 year, a final postoperative visual acuity difference of 20/96 (LogMAR 0.208) for silicone oil eyes versus 20/44 (LogMAR 0.453) for gas treated eyes.[8] Lai et al also showed the visual acuity advantage of gas tamponade with a smaller difference (20/70 vs 20/50).[9] However, Lai et al also showed the rate of single operation closure being only 65% for silicone oil and 91% for gas tamponade.[9] Thus, unless limited by patient circumstances, gas tamponade for macular hole repair is preferable to silicone oil tamponade.
Controversies surrounding the surgical repair of macular holes
20-gauge versus 23-gauge versus 25-gauge vitrectomy systems
While no one system poses a significant long-term advantage, smaller gauge vitrectomy systems, with frequently self-sealing wounds, avoid induced astigmatism from suturing sclerotomies, resulting in a more rapid recovery of vision.
An initial increase in endophthalmitis appears to have been addressed by changing the means of wound construction but may still be considered a disadvantage to small gauge vitrectomy systems.
Smaller gauge vitrectomy systems, especially 25-gauge systems, lack shaft stiffness because of the smaller barrel and also complicate the actual vitrectomy surgery for surgeons trained using 20-gauge systems.
Internal limiting membrane (ILM) peeling
ILM peeling increases the rate of hole closure 93-100%.
The rate of visual recovery was postulated to be slowed by ILM peeling, but no recent literature supports this assertion (see next bullet point).
Spiteri-Cornish et al compared peeling with not peeling ILM in a meta-analysis of 4 randomized controlled trials. The results demonstrated an effect favoring ILM peeling for macular hole closure and final visual acuity. The analysis did not identify any difference in the rate of recovery. The benefit of ILM peeling became evident even by 3 months postoperatively.[10]
Use of vital dyes
Indocyanine green (ICG) dye was the first vital dye used for macular surgery. There is considerable literature questioning the toxicity of ICG dye to the retina and retinal pigment epithelium (RPE). Despite the laboratory science and literature cautioning the use of ICG dye, an equal amount of literature documented good surgical and visual results. ICG dye is still used by surgeons with care taken to limit the exposure of the retina and, potentially more importantly, the RPE to the dye.
Trypan blue has also been used to stain the ILM without the literature suggesting toxicity. On the other hand, trypan blue does not appear to stain the ILM as effectively as ICG dye.
Triamcinolone acetonide has also been used to facilitate peeling of the ILM. As of 2008, it is the only surgical adjunct to peeling of the ILM that is FDA approved for use in the eyes.
Management of lamellar holes
Lamellar holes cause symptoms but minimal loss of central visual acuity. Management has historically been conservative.
Surgical intervention has been undertaken with vision loss or patient symptomology with the recent advances in small gauge vitrectomy and further experience with ILM peeling.
Garretson et al reported a series of successfully repaired lamellar macular holes, wherein 93% eyes demonstrated improved visual acuity.[11] The mean improvement was 3.2 Snellen lines.
Face-down positioning
Historically, strict face-down positioning had been recommended for patients for up to 4 weeks, with consequent difficulties of compliance and patient quality of life during that period.
More evaluation placed into shorter periods of face-down positioning, though, traditionally, it has been believed that the shorter the period of face-down positioning, the lower the rate of successful hole closure. In 1997, Tournambe et al described a pilot study of patients without face-down positioning. They reported a success rate with one surgery of 79% and suggested that pseudophakia was necessary for consideration of liberalization of positioning requirements.
The advent of ILM peeling has encouraged a second look at minimal to no face-down positioning. Rubinstein et al described a case series of 24 eyes of patients who underwent ILM peeling and then did not position postoperatively.[12] In this case series, 22 eyes were successfully closed and had visual improvement with both eyes that failed being stage 4 large holes.[12]
Others have reported comparable, if not better, results in patients with only 1 day of positioning. Dhawahir-Scala et al suggests that a critical factor is the size of the gas bubble on postoperative day 1 being greater than 70%.[13] Tranos et al showed, however, that there may be more rapid progression of cataract formation with less face-down positioning.[14] Tranos et al were among several authors who recommended combined phacovitrectomy for phakic patients to allow less stringent positioning requirements.[14] Iezzi and Kapoor reported a series of 68 eyes that underwent macular hole repair with broad ILM peeling and SF6 tamponade without any face-down positioning. They reported a 100% rate of closure with a single procedure.[15]
Other considerations
The use of pharmacologic adjuncts, such as a transforming growth factor-beta (TGF-beta) and autologous serum, to facilitate hole closure has not been proven to have any added benefit as compared to controls such that their use has not gained much popularity.
Morizane et al reported a series of 10 patients with refractory macular holes who were managed with autologous transplantation of ILM. These eyes represented eyes that did not respond to initial surgery with standard ILM peeling or other modifying conditions such as myopic foveoschisis or trauma. All eyes responded to this procedure.[16]
Medication Summary
The first protease to treat vitreomacular adhesions associated with macular hole was approved by the FDA in October 2012. Nonsurgical closure of the macular hole was shown in 40.6% of patients treated with an intravitreal injection of ocriplasmin compared with 10.6% who received placebo.[5] However, there is evidence of potential retinal toxicity associated with the use of ocriplasmin. Anatomic changes in the outer segments were seen in 7 of 17 patients reported in a series by Singh et al.[17] Multiple case reports have also evaluated individual patients with ancillary studies such as electroretinography and perimetry.[18] Fahim et al suggest that the retinal dysfuction associated with ocriplasmin may be related to the enzymatic cleavage of intraretinal laminin.[19]
Class Summary
Protease enzymes provide a nonsurgical treatment method for vitreomacular adhesion.
Ocriplasmin intravitreal (Jetrea)
Elicits proteolytic activity against protein components within the vitreous body and vitreoretinal interface (eg, laminin, fibronectin, collagen), thereby dissolving the protein matrix responsible for vitreomacular adhesion.
Because complications, such as cataracts and retinal detachment, can follow treatment for macular holes, regular examinations are necessary.
Surgical complications include retinal detachments, iatrogenic retinal tears, enlargement of the hole, macular light toxicity, postoperative pressure elevation, and cataractogenesis.
Postoperative pressure elevation usually can be treated pharmacologically but may sometimes require an anterior chamber or vitreous tap.
Failure of hole closure/hole reopening
Histopathologic evaluation of specimens from patients with failed initial macular hole surgery demonstrated massive proliferation of cells and newly formed collagen associated with remaining ILM. The residual ILM and the associated collagen fibrils may become the source of persistent traction that prevents macular hole closure.
Retinal detachment/iatrogenic tears
The rate of postoperative retinal detachment is reported from 2-14%. Chung et al identified that the induction of a posterior vitreous detachment during surgery was a key risk factor for the development of iatrogenic retinal breaks. They found an overall incidence of 14.6% (20 of 137 eyes) for retinal breaks. Only one retinal break (3.1%) was identified in a macular hole patient who did not require the induction of a PVD. However, only 32 of 137 eyes undergoing vitrectomy for macular hole surgery did not require this step in the procedure, owing to the underlying pathophysiology of macular holes.[20]
Visual field defects
Visual field defects have been noted following macular hole surgery.
They are related to dehydration of the nerve fiber layer.
The rate is reduced by shorter surgical times, lower air flow, and oblique placement of infusion cannulas caused by beveled incisions of smaller gauge vitrectomies.
Cataract formation
There is a small risk of hole reopening in the immediate postoperative period following cataract surgery.
Consideration of prophylaxis versus cystoid macular edema may reduce the risk of hole reopening after cataract surgery.
A retrospective case series by Bhatnagar et al (2007) suggest that prior or simultaneous cataract extraction may carry a better long-term visual prognosis than cataract extraction following macular hole repair due to the risk of reopening of the hole following cataract surgery.[21]
In 1994, Wendel reported a series of 235 consecutive eyes undergoing repair of macular holes.[22] In this series, 93% of patients were successfully managed with only a single operation; 60% patients experienced 4+ lines of visual improvement; and 84% patients experienced 2+ lines of improvement.[22] Within this group, 58% of patients achieved 20/40 or better final visual acuity.[22]
Multiple other studies cite similar success rates, though vision recovery may be protracted and also further delayed by onset of cataract formation. Use of ILM peeling may further increase the rate of single operation success, though it may potentially slow or affect final vision recovery. See Controversies surrounding the surgical repair of macular holes.
OCT imaging preoperatively and postoperatively has provided additional prognostic data for visual recovery following macular hole surgery. Factors on OCT predictive of good visual acuity macular hole surgical outcome are as follows:
-
Size of macular hole (minimum diameter < 311 µm)
-
Traction on macular hole edges as defined by various parameters (eg, macular hole height)
-
Development of a normal photoreceptor inner segment and outer segment junction, which can occur as early as 1 month postoperatively but typically by 6 months postoperatively as shown in the images below.
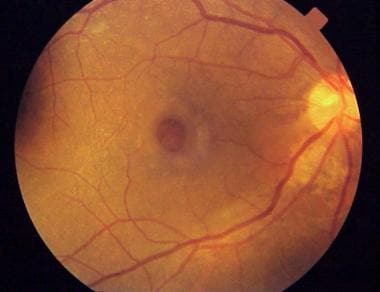
 Preoperative fundus photograph of a macular hole.
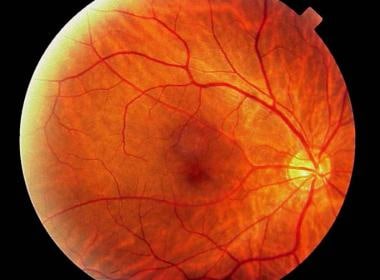
Preoperative fundus photograph of a macular hole. Fundus photograph of the same patient as in the image above at 6 months postoperatively. Note the increased media opacity caused by cataractous changes of the lens.
Fundus photograph of the same patient as in the image above at 6 months postoperatively. Note the increased media opacity caused by cataractous changes of the lens.
While surgery for macular holes is considered elective, it is important for the patient to consider prognostically that there is potentially a risk for the fellow eye to develop a macular hole as well (12%).
Older individuals should be educated on the necessity of a yearly eye examination since early symptoms of a macular hole can easily go undetected by the patient.